Before you read this article, make sure you have a read of Part 1 and 2 for frames we love, and tips and tricks to get your child into glasses!
Lens coatings and materials
When purchasing glasses at the optometrist you will be offered various optional coatings and lens thinning amonst other things, these all cost extra and therefore increase the total cost.
The advice provided below does not apply equally to everyone, but does cover the most commonly considered coatings and offers from optometrists and our view on them.
Talk to us about your child's eyes
Thinned lenses
One of the most common discussions we have with parents is around lens thinning. What does it actually mean to thin a lens? Is it worth the additional cost?
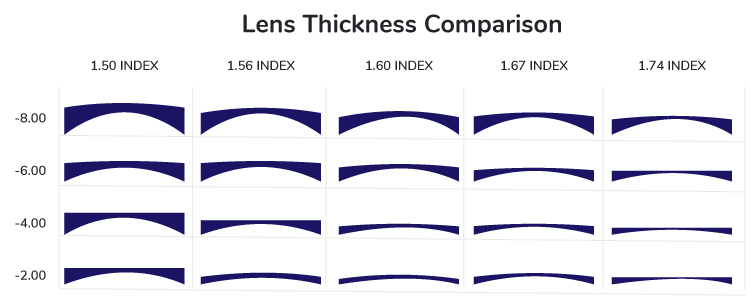
The phrase to understand here is ‘refractive index’. This phrase indicates how much the light is ‘bent’ when it goes through the glasses lens, the higher the number, the stronger the lens is and therefore the thinner the lens will end up being.
The diagram below demonstrates the commonly seen lens indexes in Australia, and how thinning effects a short-sighted (minus) prescription.
In our view, there are two main reasons to consider lens thinning in baby glasses.
Glasses lenses being too heavy for them to sit properly on the face. In these cases I start by reconsidering the frame that has been chosen, and whether it is suitable for the lens prescription provided by the ophthalmologist or optometrist. There are also basic adaptations that can be made to glasses to make them sit better on the nose.
There are times where young babies are given very high prescriptions (i.e. after cataract surgery aka aphakia) and these require special consideration compared to a standard prescription – see section on Aspheric/Lenticular lenses below.
Lenses too thick to fit into the glasses frame chosen. In this case, I make sure that there are no alternative frames that would work. Generally silicone frames are very flexible and can cope with thick lenses well.
Overall, our view is in most cases lens thinning in babies is not worth the expense due to the speed at which they grow out of each prescription. Better solutions are to change to a different frame, selecting frames with built in straps, buying a suitable ear grip/temple tip or nose pad adaptation would be a much cheaper option.
I would spend your money on a glasses frame that could potentially take up to 2 lens changes over the first year of life, so that you get the most out of the frame.
Lens Coatings
We strongly advise that parents get the anti-scratch coatings and the anti-reflective coatings on their baby’s glasses. These are worth the cost in our view.
Lens Material Types
Polycarbonate - the best option for kids
All children, no matter their age, should be given at least Polycarbonate lenses, if not upgraded to Trivex lenses
Polycarbonate has multiple fantastic qualities that make them perfect for children including:
Durable
Shatter resistant
Lightweight
UV resistant
Pre-coated with a scratch resistant layer
Polycarbonate lenses are only available as a standard 1.59 index, and therefore will not provide the thinnest lenses, but because they are lightweight this offsets the thickness and makes them work well for most children with prescriptions under +8.00 or -8.00 dioptres.
Aspheric or Lenticular Lenses
Very high glasses prescriptions in babies and children often require lenticular type glasses, potentially with an aspheric design. These types of lenses are specialist and therefore expensive, but provide good levels of vision with less distortion or aberration than a standard polycarbonate lens would.
These lenses are thinner on the edge, with the thicker lens only in the centre of the glasses lens. This makes them thinner and more lightweight.
Generally these types of glasses are seen in babies and young children who have had cataracts removed (aphakia), dislocated lenses and Stickler’s syndrome and are not suitable for contact lenses to be provided within the public health system (NB: Only in South Australia).